Relational-Cultural Theory Series Previous Articles:
What is Relational-Cultural Theory?
Transforming Community Through Disruptive Empathy
Combining the Neurobiology of Relational-Cultural Theory and Clinical Practice
By ELIZABETH (LIBBY) MARLATT-MURDOCH, LPCA, LCAS-A, CTRTC, CCTP
Since learning about Relational-Cultural theory (RCT) and relational neuroscience, they have become key components of my approach to mental health and substance abuse treatment with my clients. Using relational neuroscience in my work has been a particularly useful tool for depathologizing clients’ experiences and helping them to understand that we are hard-wired for connection with others. Elizabeth (Libby) Marlatt-Murdoch may be contacted at libbymarlatt@yahoo.com.
Your brain is shaped by your mind—including your conscious and unconscious experiences, your body, the natural world, human culture, and relationships (Hanson & Mendius, 2009). Relational- Cultural theory (RCT) is a psychological theory that acknowledges the radical power of relationship. RCT posits that throughout the lifespan, individuals grow through and toward relationship, and that culture has a profound impact on these relationships (Jordan, 2010). Relational neuroscience provides evidence that the brain is designed for connection and that without connection we cannot thrive (Banks, 2015). The neuroscience of Relational-Cultural theory offers a window into the mind and calls attention to the need to address not only an individual’s relationships in therapy, but also the social context in which they exist (Banks, 2015). Based on experience as a clinician, Relational-Cultural theory and relational neuroscience can positively impact individual outcomes in healthcare and psychotherapy as well as improve relationships and quality of life by providing a way to depathologize individual’s experiences. Sharing an understanding of relational neuroscience as it relates to RCT can be essential in promoting mutuality and growth in relationships in many areas. Multidimensional models for psychoeducation can provide key elements in accomplishing this.
Considerations and Connections
Sharing information on relational neuroscience with others can be powerful. Education is one way to begin this process. More specifically, psychoeducation, which is defined as information that is presented to individuals with a mental health condition and their families to help empower them to manage their condition in an optimal way (Bauml, 2006). So providing psychoeducation to clients about how the brain is hardwired for connection, and cannot thrive without healthy mutual connections, empowers individuals to push back against the hyper-individualistic social pressures that can undermine their health and well-being (Banks, 2015). In treatment, this knowledge can inform the process between client and clinician as they collaborate to come up with a plan to assess and improve the individual’s relational skills and to discover how previous relationships have impacted the client’s welfare. Outside of treatment, this same information may encourage individuals to evaluate their current relationships for mutuality, and provide the catalyst they need to seek more mutual relationships in an effort to improve their quality of life. The feelings of empowerment that come from this psychoeducation process can cultivate hope.
Relational neuroscience also has the power to depathologize an individual’s experience for them. In a culture that sees development as a means to independence and ignores the devastating impacts of social pain, having knowledge to educate individuals about connection as a basic need can normalize an individual’s experience of pain as it relates to social exclusion can be powerful (Banks, 2015). At the 2016 Transforming Community conference, Banks and Craddock presented their STOP SPOT model for empowering individuals to identify and address the pain of social exclusion. Social Pain Overlap Theory (SPOT) proposes that social pain which is the result of damaged or lost relationships, and physical pain which is the result of physical injury are experienced in the same part of the brain (Eisenberger & Lieberman, 2005). In the STOP SPOT model that Banks and Craddock presented at the conference, an individual must first See Stratification, then Talk and Tell their individual story related to the stratification or exclusion. The next steps they proposed are Open Outreach and finally Partnered Protest and Production.
Based on clinical experience, the ability to teach someone that his or her brain is working and responding in the way that it was designed to often results in the client or individual feeling validated. Instead of experiencing the shame or embarrassment of feeling like they are broken or their brain is broken; the client experiences a sense of safety and compassion from the therapist. This safety and compassion are necessary for the client to heal from the damage that may have resulted from relationships that are not mutual, are chronically disconnected, or in other ways are experienced as traumatic. Relational neuroscience empowers individuals by depathologizing her/his experience. This often results in increased self-compassion.
According to Walker at the Transforming Community conference, compassion is bearing witness without judgment. She also described in her ARC3 Model of Empathy that Awareness, Receptiveness, Curiosity and Courage, plus Compassion are all necessary ingredients for empathy. According to her model, Awareness is being mindful of “what is”; Receptiveness is being open to innovative and possibly conflicting knowledge; Curiosity and Courage are about embracing constructive ambiguity, vulnerability, and limitations. Relational neuroscience has the potential to depathologize a persons’ sense of self leading to less shame, which in turn opens that person up for more vulnerable relational skills of compassion and empathy. In the words of Alamaas (2016) “it is only when compassion is present that people will allow themselves to see the truth” (para. 1). The feelings of empathy and compassion that are created through the psychoeducation process can be essential for clients in working through difficult experiences and for cultivating healing and hope.
Understanding of Neuroscience in RCT
To understand the neurobiological roots of interdependence we must start with understanding the brain. The reptilian brain, also known as the brain stem, is designed for regulation of the most basic functions such as heart rate and respiration, and is also involved in rapid mobilization of the brain and body for survival (Hanson & Mendius, 2009; Siegel, 2010). The paleo-mammalian brain, also known as the limbic system, works closely with the reptilian brain stem and is designed for creating our basic drives, emotions, memory, and is essential in establishing relationships and forming emotional attachments to others (Hanson & Mendius, 2009; Siegel, 2010). And finally, the neo-mammalian brain, also known as the cortex, “represents the three-dimensional world beyond the bodily functions and survival reactions mediated by the lower, subcortical regions,” is involved in creating ideas and concepts (Siegel, 2010, p. 19). According to Banks and Craddock (2016) “being a part of a group is so critical to humans that our nervous system literally uses the same alarm (the dorsal anterior cingulate cortex) to register the distress of physical pain or injury AND social exclusion” (para. 3).
Additional evidence for this concept is provided in studies that show the link between connection and survival. Research has shown that the human brain responds in a similar way to both food and connection, that the brains of neglected orphans from World War II did not have enough neural activity to support life, and that relational trauma impacts our mental and physical health and well-being long term (Bowlby, 1969; Center for Disease Control and Prevention, 2016; Hanson & Mendius, 2009). By looking at the different levels of the brain, we can begin to gather insight into how the basic need for survival led to the development of connection as a basic need in mammals.
Relational neuroscience has the power to shed even more light on love and belonging as a basic need. In fact, the research has shown that “lasting strength comes from being centered, and held within healthy relationships” (Banks & Craddock, 2016, para. 21). Banks’ (2015) C.A.R.E. program was designed to illustrate how individuals can strengthen the neural pathways in their brains to encourage closeness and connection. In Bank’s C.A.R.E. acronym, each letter represents a quality of a healthy relationship dictated by the functioning of one of four neural pathways of connection. In this model, she describes C is for Calm which represents the feeling that you get when you have a well-toned smart vagus nerve. She also explains that when we encounter potential danger, or when we are feeling stressed, the subcortical regions (primitive brain) becomes active and helps prepare the person to deal with the threat.
According to Banks (2015), this primitive brain often makes decisions that negatively impact our relationships. She indicates having robust relationships helps to keep a person’s smart vagus nerve well-toned, which in turn makes our relationships calmer. She describes how having a well-toned vagus nerve will allow us to mediate the primitive brain’s response and prevent it from taking over; and, as a result, we are healthier and have greater mental clarity. In the C.A.R.E. model, Banks (2015) describes A is for Accepted, and represents the sense of belonging that comes when your dorsal anterior cingulate cortex (dACC) is functioning properly. This part of the brain is described by Eisenberger & Lieberman (2005) in their ground breaking work, Social Pain Overlap Theory (SPOT). Banks (2015) explains the dACC acts as an alarm for social exclusion; being chronically excluded or isolated can result in an over-reactive dACC, which means the alarm can go off even when others are welcoming. She describes R as Resonance you feel in healthy relationships, which is facilitated by the action of the mirror neuron system. She further states that when an individual’s mirroring system is healthy the individual is able to understand other’s experiences, actions and feelings by creating an internal neurological template of the same experience, action or feeling (ex. noticing you are crying while watching a movie where the characters are sad and crying). She clarifies that if the mirroring system is unhealthy, it results in the individual having difficulty understanding others and can cause difficulty for others in understanding the experience of the individual. She describes E as Energy which represents the feeling of euphoria and zest we get in healthy relationships if our brain’s dopamine reward system remains closely attached to connection. She further relates the purpose of the dopamine system is to reward the brain and body for activities that promote survival—including approach behaviors, such as mating.
Unfortunately, when individuals do not get enough dopamine from healthy relationships, they may turn to unhealthy alternatives or addictive behaviors such as using drugs, gambling, or compulsive shopping (Banks, 2015). In this case the individual is rewiring their dopamine pathway away from connection and relationships, so that even when they are in relatively healthy relationships they may not derive energy and motivation from them (Banks, 2015). In summary, the C.A.R.E. acronym combined with describing how the qualities of a healthy relationship reflect the functioning of the four pathways for connection provides a solid, basic understanding of relational neuroscience.
Models
Banks (2015) cautions that concepts of neuroscience often appear more clear than they actually are. We must always respect the complexity of the central nervous system and what we have yet to discover. When starting the process of psychoeducation as it relates to the brain, it can be helpful to begin with some basic information about the brain. For example, the brain weighs approximately three pounds and is comprised of 100 billion neurons (Hanson & Mendius, 2009). Neurons connect via synapses and get their signals from other neurons through these receiving synapses and the signal is usually a burst of chemicals called neurotransmitters (Hanson & Mendius, 2009). Neural signals represent a piece of information according to Hanson & Mendius (2009), and the mind can be defined in a broad sense as the totality of those pieces of information. It is important to recognize that no single area of the brain is exclusively responsible for regulating relationship, which means creating healthy relationships is an easier task if your central nervous system is integrated, balanced, and flexible (Banks, 2015). Every interaction an individual has with the world changes the brain in some way, and individuals are capable of neurogenesis (creating new connections in the brain) as well as neuroplasticity (altering existing connections in the brain throughout their lives) (Banks, 2015; Siegel, 2010).
Visual aids for use in psychoeducation, such as Siegel’s hand brain (2012) or van Eys’ felt brain (personal communication, July 7, 2016), allow individuals to see how the brain works so they can change what the brain does. Siegel’s hand brain (2012) provides a portable and accessible brain model for neurologists and clients alike. His model is quite simple to create: take your thumb and fold it in towards your palm, then put your fingers over the top. He describes how the wrist represents the spinal cord, the palm represents the brain stem, the thumb folded inward onto the palm represents the limbic system, and the fingers covering the thumb represent the cortex.
To understand how the brain works, it is helpful to differentiate between parts of the brain that we have conscious control of from those we do not. In Siegel’s hand brain model (2012), if you raise your four fingers then you separate these two areas. He describes the four raised fingers as representing the cortex which is the part you have conscious control over. He elaborates that the thumb folded over the palm represents the subcortical regions that are beyond our direct conscious control. The importance of this distinction can be further emphasized by pointing out that the fear activation response takes 50 milliseconds, which is about 1/20 of a second, whereas conscious thought takes 500-600 milliseconds, or half a second (Cozolino, 2010).
Using Siegel’s hand brain model (2012), you can get a visual understanding of the first component of the C.A.R.E. program—Calm. He illustrates the process of “flipping our lids” by unfolding the fingers that were covering the thumb and palm to expose the rest of the hand which represents the limbic system and brain stem. When a person is triggered, the individual’s primitive brain is responding without the protective inhibition of the cortex—the logical/rational part of the brain (Banks, 2015). When this happens, Banks (2015) indicates the individual’s brain is not experiencing the feeling of calm that results when the individual can use their well-toned smart vagus nerve to mediate the response of the primitive brain. The Siegel hand brain model (2012) can be taken one step further by showing clients the location of the vagus nerve which runs between the right hemisphere (right two fingers) and left hemisphere (left two fingers) of the brain down through the limbic system and (via the parasympathetic nerve) into the brain stem and the rest of the body. Providing a visual representation of the location of the vagus nerve can increase understanding for the client about the role a well-toned smart vagus nerve has in calming both the brain and the body. In simple terms, when an individual has good smart vagal tone, they are able to accurately read a situation or person as safe and respond with engagement behaviors that result in enhanced connections and mutuality in relationships (Banks, 2015).
The second component of Banks’ C.A.R.E. program (2015), Accepted, involves the dorsal anterior cingulate cortex which is located deep in the frontal cortex, and can be illustrated using the hand brain model by showing the underside of the two middle fingers (Siegel, 2012). In Siegel’s hand brain model (2012), the two middle fingers represent the middle prefrontal cortex, which includes the dACC. It is important to emphasize that the dACC is part of an alarm system that responds to physical pain and injury as well as social exclusion, both of which are dangerous if left unaddressed (Banks, 2015). Both individual relationships and culture can impact our dACC explains Banks (2015). Developmental models that focus on independence and promote interpersonal competition often stratify and judge human differences creating an over reactive dACC, and consequently reactive pain pathways (Banks, 2015; Banks & Craddock, 2015).
The third component of Banks’ C.A.R.E. program (2015), Resonance, reflects the functioning of the mirror neuron system which is located in the parietal, frontal, and temporal lobes. In Siegel’s hand brain model (2012), the four fingers represent the cortical areas of the frontal and parietal lobes while the thumb represents the temporal lobe where the amygdala is located. It can be helpful to explain that the area of the cortex (four fingers) that is activated depends on the particular behavior or feeling that is being mirrored (Banks, 2015). In the hand brain model, Siegel (2012) indicates that the fingers overlap the thumb and palm illustrating how mirrored messages are created in the cortical areas and then transferred downward into the limbic system, then into the brain stem, and on into the body. He clarifies that these messages are transferred via the insula, also known as the “information superhighway” between the mirror neurons areas and the subcortical regions of the brain. The existence of the mirror neuron system is further evidence that we are biologically hardwired and evolutionarily designed to be interconnected (Banks, 2015). In fact, individuals understand what others are thinking and feeling by imitating them internally (Banks, 2015).
The final component of Banks’ C.A.R.E. program (2015), Energy, involves the social motivation system/dopamine reward system. This is located in the mesolimbic dopamine pathway, which travels from the brainstem through the limbic system, into the anterior cingulate gyrus and orbitomedial prefrontal cortex (Banks, 2015). This pathway can be identified on Siegel’s hand brain model (2012) by placing the pointer finger of your free hand on the palm of the hand brain model, moving it up to and through the thumb and ending at the fingers that represent the cortex.
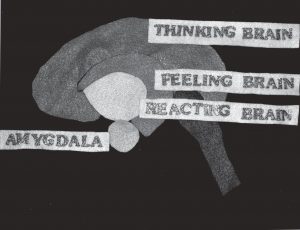
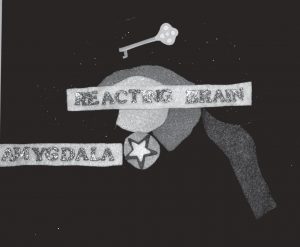
Figure 1: Van Eys’ Felt Brain or Brain Puzzle
Another model or visual aid for making Relational Neuroscience accessible to clinicians and clients is the van Eys’ felt brain (personal communication, July 7, 2016), also referred to as the Brain Puzzle (see Figure 1). She indicated that this model was designed to create a basic understanding of the brain and its functions and to illustrate and facilitate an understanding of the body’s alarm system response. She described the felt brain as made of several pieces of felt: a large blue piece of felt shaped like the cortex labeled “thinking brain”; a pink piece of felt shaped like the brain stem added to the bottom right of the cortex; pieces of green felt and orange felt labeled “feeling brain” and representing the limbic system placed directly under the cortex and in front of the brain stem; a light orange almond shaped piece of felt represents the amygdala which together with the limbic system and brain stem is labeled “reacting brain”. She indicated that a felt star is used as a visual representation of a trigger and is placed over the top of the amygdala. She further explained that after the star has been placed over the amygdala a black piece of felt shaped like the cortex is placed over the top of the cortex to represent the idea that the cortex is not online during an amygdala highjack. This model, much like Siegel’s hand brain (2012), can be used to communicate a wealth of information about neuroscience, including RCT’s relational neuroscience. The felt brain model can be used to communicate the elements of the C.A.R.E. program in much the same way that the hand brain model was adapted.
Both of these models can be used in an interactive way. Clinicians can ask their clients to mirror the movements of the hand brain and/or work with their client to assemble the Brain puzzle. The felt brain model described by van Eys (personal communication, July 7, 2016) was created by van Eys and Tisthammer in 2015 and also includes a script containing informal language interspersed with scientific terms that makes the script easy to read and easy to follow. Their script even includes opportunities for discussion, encourages the user to change it in any way that makes sense for the audience, and even explains an amygdala highjack—which is the same principle discussed in the first component of Banks’ C.A.R.E. program (2015), Calm. This script by Van Eys and Tisthammer (personal communication, July 7, 2016) states in part:
Now, the limbic system cannot think…it can only feel and react. Only the blue part, the thinking brain, can think. Sometimes, the limbic system gets a danger signal and it gets afraid. It feels and reacts. So the brain’s alarm goes off because the reacting brain recognizes danger. So, let’s put this red star on the amygdala to show that the brain got that kind of danger signal. Let’s call this the “amygdala alarm.”
When the alarm goes off, the brain sends out chemicals that give our body energy to cope with danger (or “to handle the danger in order to get safe”). Our hearts beat faster, we breathe more rapidly, there is more energy sent to our muscles so that we can fight or run away from the danger. Or sometimes, we freeze or hide so that the danger won’t come to us.
Here’s an important thing: only the parts of our brain that help us survive are working when the amygdala alarm goes off. The other parts of the brain shut off until we have learned that we are safe; we will talk later about how we can recognize “triggers” so that we can quickly know that we are safe and turn the alarm off. The thinking part of the brain isn’t working because it isn’t needed at this time. (p. 7-8) There are a number of things that may be taken from these two multidimensional models that can make relational neuroscience more accessible to practitioners.
- First, simplify the concepts of neuroscience appropriately in order to more effectively educate others.
- Second, build a foundation for understanding by introducing the intended audience to fundamental facts about the brain by using basic language to convey the message.
- Third, think outside the box and adapt existing visual aids or models to work for a new objective—in much the same way that the hand brain and felt brain models have been adapted to provide psychoeducation on relational neuroscience.
- Fourth, promote understanding by asking open-ended questions, gathering feedback, and experimenting with interactive methods instead of just using the model as a visual aid.
- Finally, use caution in deciding when it is appropriate to use relational neuroscience with clients or other individuals; this comes from experience and the ability to be attuned to those we serve.
 The importance of sharing relational neuroscience with our clients has been supported by a number of considerations based on the tenets of Relational-Cultural theory. Psychoeducation on relational neuroscience has the ability to empower the individual to make changes in addition to depathologizing and validating the individual’s experience. This can often result in increased levels of compassion and empathy necessary to be with the pain that can result from relational trauma, loss, exclusion and/or isolation. Learning and sharing relational neuroscience represents a practical opportunity to enhance well-being, develop compassion, and reduce suffering through cultivating healing and hope.
The importance of sharing relational neuroscience with our clients has been supported by a number of considerations based on the tenets of Relational-Cultural theory. Psychoeducation on relational neuroscience has the ability to empower the individual to make changes in addition to depathologizing and validating the individual’s experience. This can often result in increased levels of compassion and empathy necessary to be with the pain that can result from relational trauma, loss, exclusion and/or isolation. Learning and sharing relational neuroscience represents a practical opportunity to enhance well-being, develop compassion, and reduce suffering through cultivating healing and hope.
References
Alamaas, A. H. (2016) Compassion leads to the truth. Retrieved from: http://www.ahalmaas.com/glossary/compassion
Banks, A. (2015). Wired to connect: The surprising link between brain science and strong, healthy relationships. New York: Penguin.
Banks, A., & Craddock, K. (2016). Stopping the pain of social exclusion. Retrieved from: https://www.wcwonline.org/News-Events-Extra-Information/full-article-stopping-%09the-pain-of-social-exclusion-full-blog-article
Bauml, J. (2006). Psychoeducation: A basic psychotherapeutic intervention for patients with schizophrenia and their families. Schizophrenia Bulletin, (32)1.
Bowlby, J. (1969). Attachment and loss (Vol. 1). New York: Basic Books.
Center for Disease Control and Prevention. (2016). About adverse childhood experiences. Retrieved from: https://www.cdc.gov/violenceprevention/acestudy/about_ace.html
Cozolino, L. (2010). The neuroscience of psychotherapy: Healing the social brain (2nd ed.). New York: W.W. Norton & Co.
Eisenberger, N.I. & Lieberman, M.D. (2005). Why it hurts to be left out: The neurocognitive overlap between physical and social pain. In K. D. Williams, J. P. Forgas, & W. von Hippel (Eds.), The social outcast: Ostracism, social exclusion, rejection, and bullying (pp. 109-127). New York: Cambridge University Press.
Hanson, R., & Mendius, R. (2009). Buddha’s brain: The practical neuroscience of happiness, love & wisdom. Oakland, CA: New Harbinger Publications.
Jordan, J. V. (2010). Relational cultural therapy (1st ed.). Washington, DC: American Psychological Association.
Siegel, D. (2012). Dr. Daniel Siegel presenting a Hand Model of the Brain. Retrieved from https://www.youtube.com/watch?v=gm9CIJ74Oxw
Siegel, D. J. (2010). Mindsight: The new science of personal transformation. New York: Bantam Books.